A 30-year-old patient came to my office with a problem that traditional surgery would have solved by scraping or re-operating on the cornea. She had a scar, what we call a leukoma, in her left eye, and she saw halos and glare every night while driving. We cleared it without going back to the operating room, with a medication that most people associate with blood pressure: losartan, this time as eye drops. In March 2024, at the Faco-Caribe Congress in Barranquilla, I presented precisely the use of topical losartan for corneal fibrosis, and this case is a concrete example of what I see in practice.
Let me be honest from the start. Topical losartan for the cornea is an off-label use, outside its approved indication, prepared as a compounded formulation, and still an emerging line of management. It is not a standard treatment or a universal solution. It is one more option, available for selected cases and under the supervision of a cornea specialist.
What haze is and why a scar appears in the cornea
The cornea is the transparent window of the eye. When we operate on its surface, as in a surface ablation such as PRK, that transparency depends on the cornea healing in an orderly way. In some eyes, the repair gets out of control and haze appears, a cloudiness that, in its most marked form, organizes into a scar or leukoma.
What happens underneath is an exaggerated healing response. The cells that keep the cornea's collagen orderly, the keratocytes, transform into myofibroblasts and lay down tissue in an irregular way. That irregularity is what scatters light, and that is why the patient reports halos, glare, and a quality of vision that glasses cannot fully clean up.
Not every eye reacts the same way. Significant haze is uncommon with today's techniques and care. Its incidence after a surface ablation dropped to around 1% once mitomycin C began to be used during surgery, when it used to be much higher. But when it does appear, it conditions the vision of a young person who had surgery precisely to see better. That is the scenario we faced here.
The case: nighttime glare that would not ease
The patient had myopic astigmatism and, in 2023, had undergone surface refractive surgery combined with crosslinking, an approach along the lines of the so-called Athens Protocol, to correct her prescription and reinforce the biomechanics of the cornea. The surgery met its refractive goal. The problem came afterward.
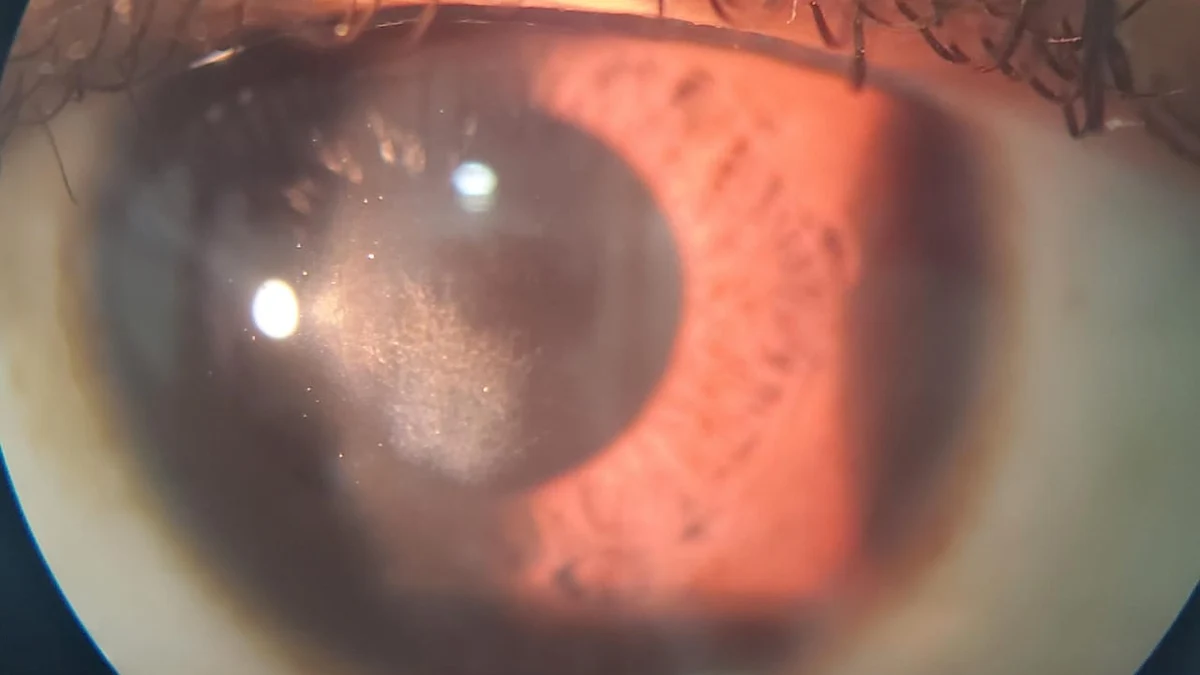
During follow-up she developed a paracentral leukoma, located in the inferonasal part of the left eye. Her main complaint was not distance or near vision, but night: glare and discomfort with lights while driving, that halo phenomenon that appears when the pupil dilates in the dark and uncovers the area of the cornea that is not perfectly transparent.
In the office, the refraction confirmed what she felt. Uncorrected, her vision had dropped, and although it improved with lenses, the scar kept scattering light. The classic option in a case like this is surgical, removing or polishing the scar. Before that, the protocol I follow includes exhausting medical management, because every additional surgery on an already operated cornea carries its own cost.
Why losartan, and how it acts on the scar
Losartan is known as a blood pressure drug, from the family of angiotensin receptor blockers. Its interest in the cornea comes from another place. In corneal healing studies, done mostly in animal models and in a still limited number of human cases, losartan has behaved as an antifibrotic because it modulates the TGF-beta signaling pathway, the signal that pushes keratocytes to become myofibroblasts and to lay down scar tissue. By dampening that signal, a scar that is already there can remodel and clear.
Much of that research comes from the laboratory of Dr. Steven Wilson, at the Cole Eye Institute of the Cleveland Clinic, with support from research institutes in the United States and the collaboration of Brazilian ophthalmologists such as Dr. Marcony Santhiago. It is still evidence in development, and that is why I insist on the framing: this is an experimental use, not a consolidated standard.
What I find clinically relevant is the change in logic. Instead of removing the scar mechanically, we act on the biological process that sustains it. In my experience, when that approach works, it avoids a surgery and restores transparency to the cornea in a more physiological way.
The treatment and how it evolved
In this case I combined three drops with different goals. Topical losartan, at low concentration, as the antifibrotic meant to remodel the scar. A corticosteroid, loteprednol, alongside it to control the inflammation of healing. And a third drop, brimonidine, with a more practical function: it slightly reduces the pupil diameter, so that in dim light the pupil does not fully uncover the scarred area, which eases the nighttime symptoms while the tissue improves.
The treatment was maintained for around three months, with serial clinical and photographic follow-up, because the remodeling of a scar is not judged by a single visit, but by the trend from one photo to the next.
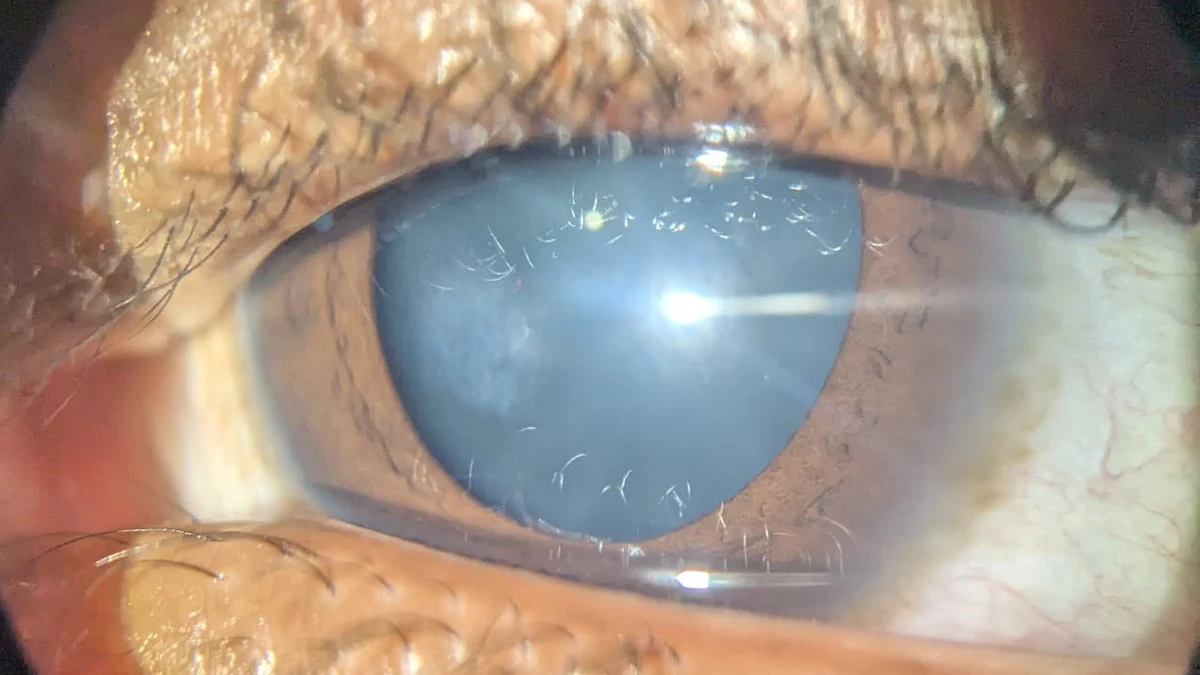
At the control evaluation, the result was the one we were looking for. Uncorrected vision settled around 20/25 in both eyes, and with a minimal prescription it reached 20/20. More important to her, the nighttime symptoms had disappeared. On slit-lamp examination, the paracentral leukoma looked much fainter, with a clear improvement compared with the earlier images. From there, the plan was to withdraw the brimonidine and leave only lubrication, with no need for any additional refractive treatment, because the residual astigmatism was minimal and not visually significant.
Who it may make sense for, and who it does not
This approach does not replace surgery in every case, and it is not for every scar. It makes more sense when the scar is relatively recent and still biologically active, that is, when there is a process that can be modulated, and when the patient and the physician prefer to exhaust medical management before re-operating. This depends on the case, and the decision is made by the specialist who examines the cornea in person.
Beyond haze after refractive surgery, the same antifibrotic principle has been documented in isolated cases for other corneal scars. Among them, the haze that appears after crosslinking, reported in the journal Cornea, and some leukomas left as a sequela of herpes or varicella zoster keratitis, where a short case series showed a good response. In scars from pterygium surgery, by contrast, the only published case did not improve, so there is no evidence that losartan is useful there. In almost all of these scars the enemy is the same, a fibrosis of the stroma that used to be addressed only by scraping or transplanting.
I prefer to present it with caution. It is one more tool in the management of the complex cornea, not a promise. Its value is that, in the right patient, it can avoid a surgery and preserve tissue, which in the cornea is always the most valuable thing.
Frequently asked questions
Are losartan eye drops an approved treatment for the cornea?
Not as such. Losartan is approved for blood pressure, and its topical use in the cornea is off-label, prepared as a compounded formulation, within a line of management that is still emerging. That is why it is only considered in selected cases and under the supervision of a cornea specialist.
Does it work for any scar in the eye?
No. It tends to make more sense in relatively recent and active scars, where the fibrosis process can still be modulated. Very old, consolidated scars respond less, and some cases still require surgery. It is an individual assessment.
How long does it take to see a result?
In this case the follow-up was around three months, with serial photographic checks. The remodeling of a scar is gradual, so the criterion is not a single visit, but the trend of improvement over the weeks.
Is haze after refractive surgery common?
Significant haze is uncommon with today's techniques and care, but it can happen. When it appears and affects vision, there are management options, from medical treatment to surgery, depending on the case.
Did the patient have to be operated on again?
No. The goal of the treatment was precisely to avoid another surgery on an already operated cornea, and in this case we managed to clear the scar and resolve the symptoms with medical management alone.
When biology solves what the scalpel used to
Cases like this sum up where corneal management is heading. For years, a scar in the stroma had two paths, scraping it or transplanting. Today, in the right patient, we can act on the biological process that sustains it and give the cornea the chance to clear on its own. It is the same philosophy with which, in other cases, we have been able to rescue a cornea without reaching a transplant by relying on medical management: preserving the tissue whenever possible.
If you had refractive surgery and were left with halos, glare, or a haze that glasses do not correct, it is worth a specialized cornea evaluation before assuming that the only way out is to return to the operating room. You can write to us for an assessment and review, with your case in hand, which options make sense.


