For most patients, cataract surgery means seeing clearly again. So when someone leaves the operating room with a new intraocular lens and still cannot reach the vision they expected, the first reaction is usually to assume that something went wrong with the operation. In a subset of these cases the problem is not the cataract or the lens that was implanted. It is the cornea, and sometimes a diagnosis no one had made.
This case illustrates it well. A 70-year-old woman came to my office in April 2026 unhappy with her vision. She had undergone cataract surgery in both eyes, with intraocular lens implantation, about two years earlier at another center. The surgery itself was fine, but her best corrected vision did not exceed 20/30 in either eye. When we studied the cornea with tomography, the real cause appeared: bilateral keratoconus that had never been diagnosed.
Keratoconus is not a rare disease. The classic figure places it at around 1 in 2,000 people, although more recent epidemiological studies suggest it is considerably more common, up to nearly 1 in 375, and in its mild forms it can go undetected for years. In my experience, it is one of the diagnoses most easily missed when vision "just doesn't clear up" after intraocular surgery.
Why you can see poorly after a "successful" cataract surgery
It is worth separating two things that are often confused. One is that the cataract surgery was technically correct. The other is that the eye achieves excellent vision. They almost always go together, but not always, because the final visual result depends on the entire optical system of the eye, not only on the lens that replaces the cataract.
When a patient sees less than expected after surgery, the list of possible causes is well known. It may be an opacification of the posterior capsule, the membrane that holds the lens and that sometimes becomes cloudy over time. It may be significant dry eye, which degrades the surface through which light enters. It may be a problem of the retina or the optic nerve. And it may be, as in this case, an irregular cornea.
The cornea is the eye's first lens and provides much of its focusing power. If its surface is irregular, the image reaching the retina is distorted no matter how perfect the intraocular lens placed inside. That is why, when best corrected vision stalls at 20/30 without a clear explanation in the retina or the lens, in my judgment the cornea must be examined in detail. That was exactly the step that had been missing in this patient.
The detail that changed the diagnosis: corneal tomography
At the initial evaluation, the refraction of the right eye carried a high astigmatism, 3 diopters, and even with the best possible correction vision did not exceed 20/30. That pattern, a large astigmatism that cannot be fully corrected with lenses, is a warning sign. Regular astigmatism is corrected well with glasses; irregular astigmatism is not. And irregular astigmatism is the signature of a diseased cornea.
To see it clearly we performed a corneal tomography with the Pentacam, a study that maps the shape and thickness of the entire cornea, not just its surface. The result was conclusive: a characteristic inferior steepening in both eyes, with several altered indices consistent with corneal ectasia, more advanced in the right eye. In other words, bilateral keratoconus. The patient had had it for years, probably in a mild form that had gone unnoticed, and the cataract surgery had been planned without that information.
Here is a lesson I repeat often: an undiagnosed keratoconus before cataract surgery complicates the intraocular lens calculation and usually leaves a residual refractive error, in addition to the irregular astigmatism inherent to the disease. It is not the fault of a poorly chosen lens. It is a cornea that was not giving all the information when the calculations were made. The numbers confirm what we see in the office: when the cornea is the problem, the solution also has to go through the cornea.
What keratoconus is and why it sometimes goes unnoticed
Keratoconus is a disease in which the cornea, which normally has a rounded and regular shape, thins and bulges progressively, taking on a more conical shape. That deformation introduces irregular astigmatism and increases what we call higher-order aberrations, in particular coma, a distortion that makes points of light appear as small comet tails. The patient describes it as ghost images, halos, or vision that glasses improve only up to a point.
Advanced forms are obvious. The problem lies in the mild forms, which can give acceptable vision for years and be confused with simple astigmatism. Many of them are only discovered when a tomography is done for another reason, for example when evaluating someone for refractive surgery or, as here, when looking for why a cataract surgery did not deliver as expected. That is why I insist so much on studying the cornea before any planned eye surgery.
One point that reassures older patients: at 70 years of age keratoconus is usually stable. The disease progresses mostly in adolescence and youth, and tends to stop over the years. This is clinically relevant because it changes the goal of treatment. In a young person with progressive keratoconus, the priority is usually to halt the progression. In a patient of this age, with an already stable cornea, the priority is not to halt anything, but to regularize the cornea to recover vision. And for that the resource I chose was CAIRS.
Why I chose CAIRS and not a synthetic ring
Intrastromal segments are small arcs placed within the thickness of the cornea to modify its curvature. Inserted in the right zone, they flatten and regularize the ectatic cornea, which reduces astigmatism and can improve vision. The idea is not new; what has changed is the material.
For years, these segments were always made of a plastic called PMMA. These are the classic synthetic rings, the ICRS. They work, but the eye recognizes them as a foreign body, and over time some patients develop complications such as extrusion, migration, or deposits around the segment. CAIRS are the evolution of that concept: instead of plastic, segments carved from human donor corneal tissue are used. The underlying difference is biocompatibility. ICRS are plastic that the eye tolerates as foreign; CAIRS are human tissue that integrates with the patient's own stroma.
That integration is why, in my practice, I adopted CAIRS from its earliest stages and today it is my preferred option for many of these cases. Offering it, however, depends on something not every center has: access to quality donor corneal tissue. As Medical Director of the Eye Bank of the Dominican Republic, I have direct access to that tissue and its preparation, which makes it feasible to plan a CAIRS without depending on external availability. If you would like to understand this technique in depth, I explained it in detail in the article on CAIRS and how they differ from synthetic rings.
There is a detail that makes this case special. The usual approach, when a patient needs cataract surgery and CAIRS, is to do the segments first to regularize the cornea and then calculate the lens over an already stabilized cornea, as in the first case we operated in that sequence, with the lens placed after CAIRS. Here the sequence was the reverse: the patient had already had cataract surgery, and the CAIRS was done afterward. It was the first case in my practice in which I placed allogenic segments after cataract surgery, a different scenario that forces you to think about the goal in another way, because it is no longer about preparing the cornea for a lens, but about rescuing the vision of an eye that already has the lens in place.
How the procedure went
The tunnel within the cornea, where the segment sits, I created with the VisuMax femtosecond laser. This laser allows the channel to be carved with micrometric precision and at the exact depth planned, which is key for the segment to be well positioned and act where it should. Over that tunnel I implanted a symmetric allogenic segment in the lower part of the cornea, which is where the bulging of the cone was.
One aspect of the planning deserves explanation. By flattening the lower zone of the cornea, a segment tends to shift the refraction toward hyperopia. So that this effect would not be excessive and would not leave the patient with too much "plus," I used a slightly wider optical zone. It is a customization adjustment: each cornea responds differently, and the diameter and position of the segment are chosen according to the specific case. The procedure was performed in May 2026 without complications.
The result at one month
At one month after surgery, the right eye's cornea had changed shape measurably. The tomography showed an inferior flattening of about 3 diopters and a significant regularization of the corneal astigmatism. In refractive numbers, the astigmatism of the right eye went from 3 diopters to 0.75, an important drop that reflects a much more ordered cornea than before.
| Parameter (right eye) | Before | One month after CAIRS |
|---|---|---|
| Refractive astigmatism | −3.00 D | −0.75 D |
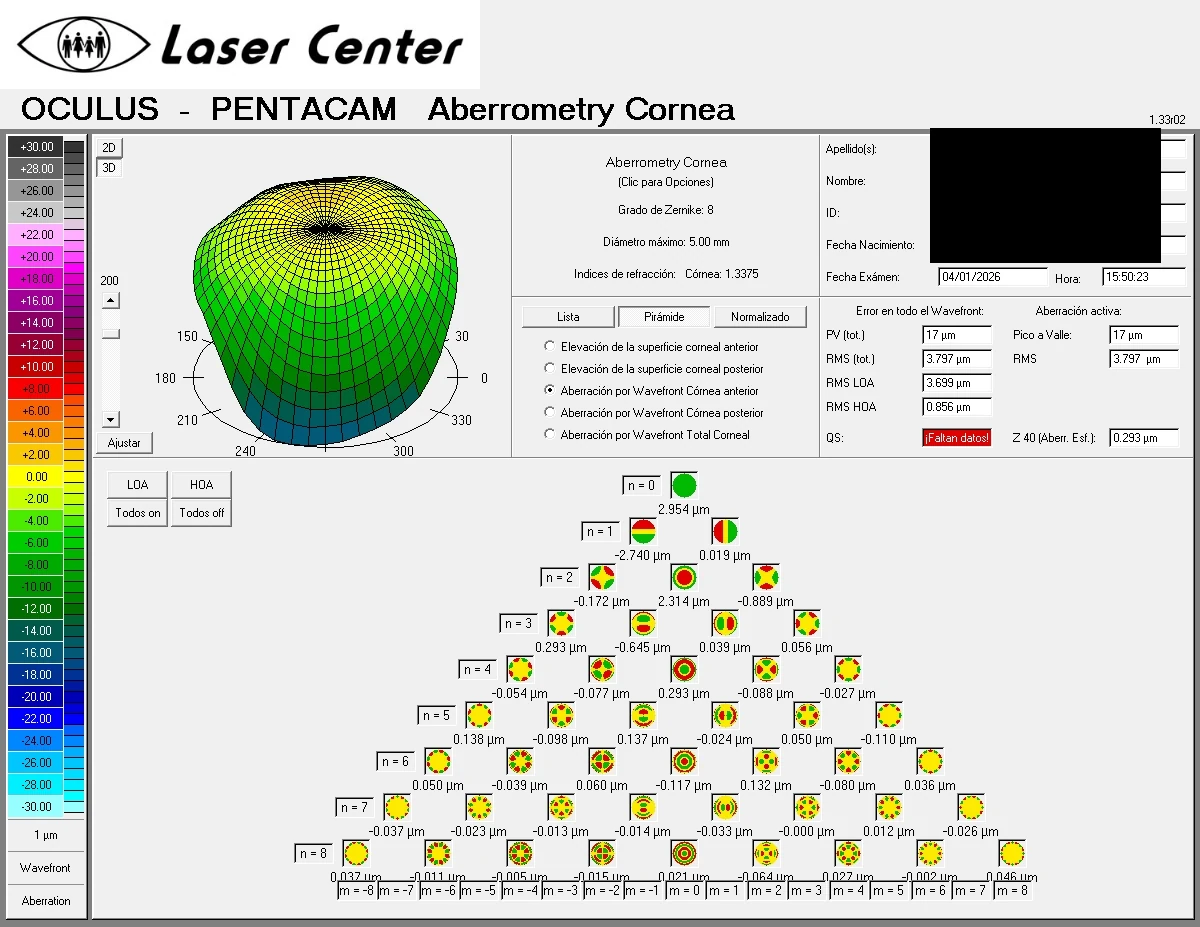
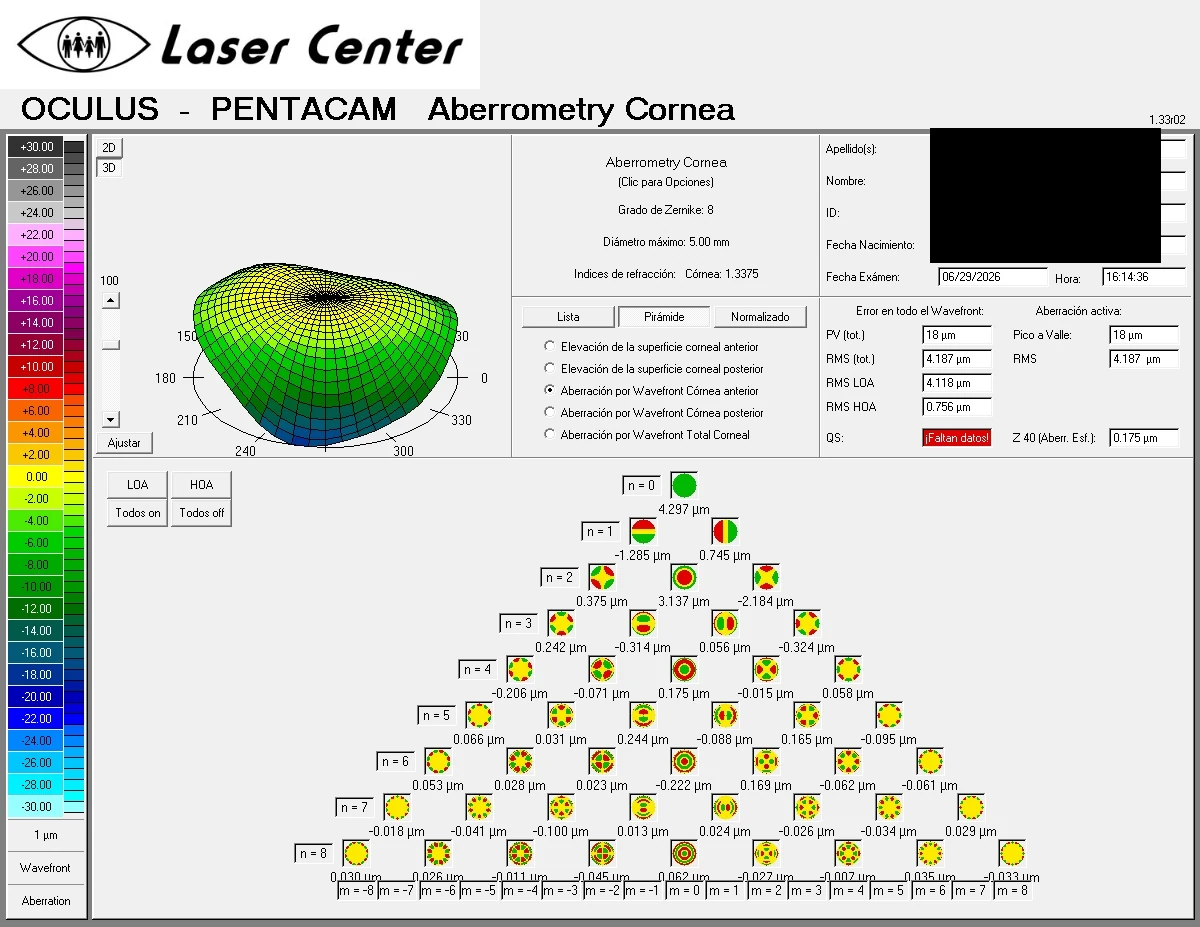
| Corneal spherical aberration | 0.293 µm | 0.175 µm |
| Best corrected vision | 20/30 | 20/30 |
| Near vision (with add) | J3 | J1 |
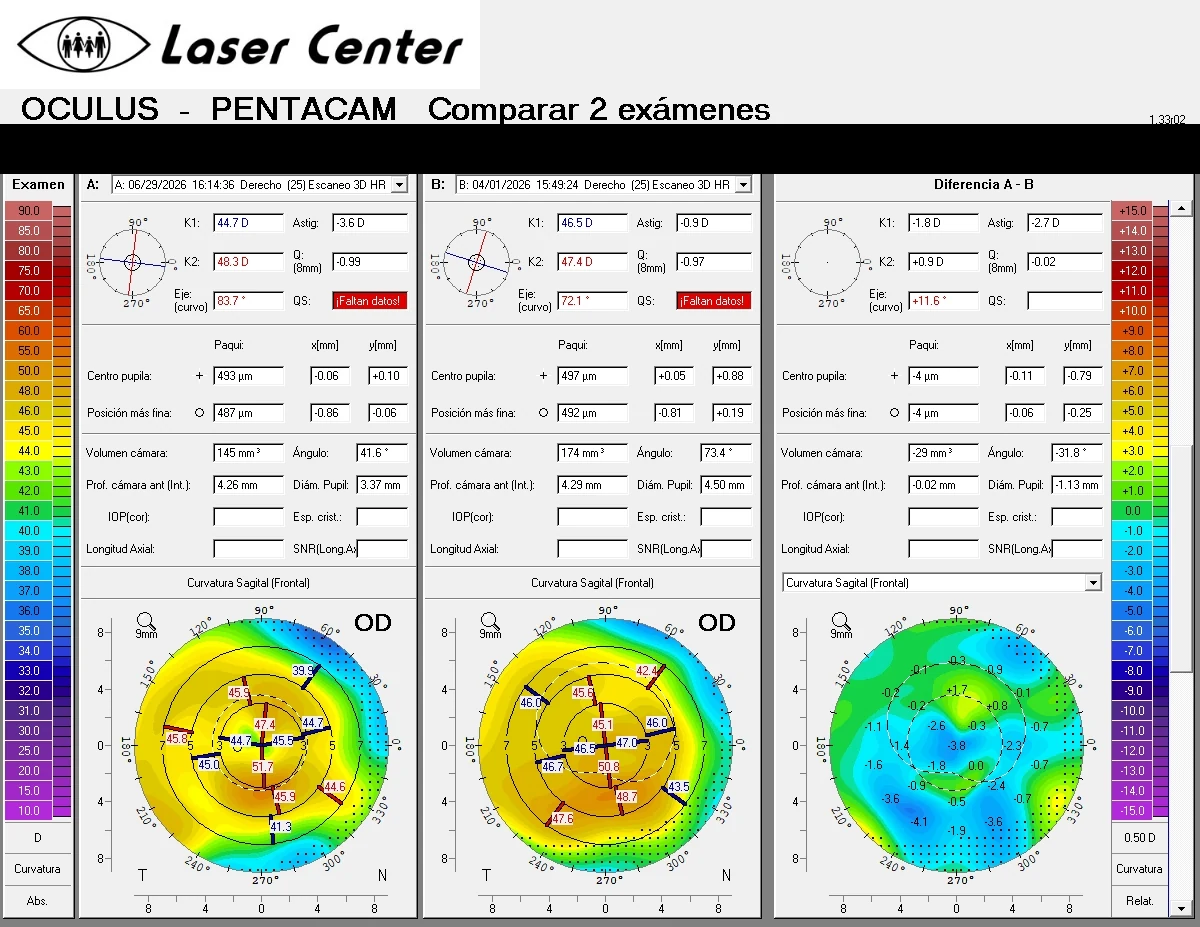
The corneal aberrometry told the same story from another angle. Comparing the previous study with the follow-up one, a reduction of spherical aberration and vertical coma was observed, that is, of those higher-order distortions that degrade visual quality in keratoconus. When those aberrations drop, the image the cornea forms is cleaner, even if the line of letters the patient reads does not always fully capture it.
I want to be transparent about what this first month means. The corrected vision of the right eye was still 20/30, but on a radically more regular cornea and with a much more manageable refraction. The CAIRS did its part, which was to regularize. The next planned step is a topography-guided custom excimer laser ablation, in both eyes, to polish the residual astigmatism and turn that already ordered cornea into better uncorrected vision. It is a two-stage strategy: first you regularize with the segment, then you fine-tune with the laser. The combination of the two techniques is a strategy that yields consistent results when executed in the correct order. For near vision, with a +2.50 add, the patient already reached J1 in both eyes, which is fine, comfortable reading.
An important detail: the other eye improved without surgery
There is a fact in this case that I use a lot to explain something to patients. The left eye, which I did not operate on, also improved its refraction. It was not caused by the segment in the other eye. It was the result of treating the ocular surface intensively with lubrication.
A dry cornea is a cornea that performs below its capacity. The tear film is the first surface light passes through, and when it is altered, vision fluctuates and worsens. Optimizing that surface, something as seemingly simple as a good lubrication plan, sometimes recovers lines of vision without touching the eye with a scalpel. Before proposing any procedure, the protocol includes putting the ocular surface in its best possible state, because part of the problem can be solved there. This left eye is the proof.
What this case teaches
If I had to sum up the message of this case in one sentence, it would be this: when vision does not follow after cataract surgery, you must study the cornea before considering the result final. In this patient, a tomography revealed a keratoconus that had gone undiagnosed for years and that explained why her vision had fallen short. Identifying the real cause made it possible to offer a targeted solution, instead of assuming that "this is how it was going to stay."
It also shows the value of individualizing. I did not use just any segment or a standard technique, but donor tissue instead of plastic, an optical zone adjusted to control hyperopization, and a two-stage plan that combines the segment with a later laser. It is not a universal solution. It is an option available for the right patient, supported by access to the tissue and by the experience of having done many of these cases. If you are interested in the full landscape of options for the cornea, you can review our cornea and refractive surgery services.
Seeing clearly again after believing there was nothing more to be done is one of the most rewarding things about this subspecialty. And it almost always begins with a correct diagnosis.
Frequently asked questions
Why do I see poorly if my cataract surgery went well?
A technically correct cataract surgery does not guarantee perfect vision, because the result depends on the whole eye. The most common causes of seeing less than expected are posterior capsule opacification, dry eye, retinal or optic nerve problems, and an irregular cornea such as keratoconus. A complete examination, including a study of the cornea, allows the specific cause to be identified.
What is keratoconus and why wasn't it detected before?
It is a disease in which the cornea thins and bulges, generating irregular astigmatism and poor visual quality. In its mild forms it can give acceptable vision for years and be confused with ordinary astigmatism, so it is sometimes only discovered when a corneal tomography is done for another reason. It is not always looked for before cataract surgery, and that is where it can go unnoticed.
What is the difference between CAIRS and synthetic rings?
Synthetic rings, or ICRS, are made of a plastic that the eye recognizes as a foreign body. CAIRS are segments carved from human donor corneal tissue, which integrates with the patient's own cornea. That biocompatibility is their main advantage and reduces certain complications associated with the synthetic material.
Can CAIRS be placed if I already had cataract surgery?
Yes. Although the usual approach is to place the segments before cataract surgery to better calculate the lens, it is also possible to do it afterward, as in this case, when a keratoconus that was limiting vision is detected. The individual evaluation determines whether the eye is a candidate and what goal to pursue.
Does CAIRS cure keratoconus?
No. CAIRS regularizes the cornea and improves vision, but it does not eliminate the underlying disease. It is a visual rehabilitation tool. In young patients with keratoconus that is still progressing, crosslinking is also considered to stabilize the cornea, something that in older patients, with the disease already stable, is usually not necessary. The decision always depends on the case.
Legal disclaimer
This content is for educational and informational purposes. It does not replace professional ophthalmologic consultation, diagnosis, or treatment. The management of keratoconus and the indication of corneal segments (CAIRS), crosslinking, or laser surgery must be defined and supervised by an ophthalmologist specializing in cornea. The results described correspond to a specific patient and may vary according to the clinical conditions of each person. If your vision is not what you expected after cataract surgery, consult a specialist for a complete evaluation.
References
- Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297-319.
- Godefrooij DA, de Wit GA, Uiterwaal CS, et al. Age-specific Incidence and Prevalence of Keratoconus: A Nationwide Registration Study. Am J Ophthalmol. 2017;175:169-172.
- Santodomingo-Rubido J, Carracedo G, Suzaki A, et al. Keratoconus: An updated review. Cont Lens Anterior Eye. 2022;45(3):101559.
- Jacob S, Patel SR, Agarwal A, et al. Corneal Allogenic Intrastromal Ring Segments (CAIRS) Combined with Corneal Cross-linking for Keratoconus. J Refract Surg. 2018;34(5):296-303.
- Vega-Estrada A, Alio JL. The use of intracorneal ring segments in keratoconus. Eye Vis (Lond). 2016;3:8.
- Parker JS, van Dijk K, Melles GRJ. Treatment options for advanced keratoconus: A review. Surv Ophthalmol. 2015;60(5):459-480.
- Savini G, Hoffer KJ. Intraocular lens power calculation in eyes with previous corneal refractive surgery and irregular corneas. Eye Vis (Lond). 2018;5:18.
Last updated: July 1, 2026